{kind=image}
{kind=image}
Thinking Beyond "Health and Wellness”
by MacKenzie Twardus, Associate Principal, Planner + Landscape Architect
By treating mental wellness with the same rigor as physical health, design becomes a tool for healing.
Have you ever presented a project where the overarching goal or primary objective was “to improve health and wellness”? What did that mean to you? Was your project focused on the physical, social, or mental dimensions of how people experience the built environment? Or was it all the above? Are you even sure, now that we’re talking specifically?
In 2022, I started working on a master plan for Crownsville Hospital Memorial Park in Maryland. Originally founded as The Maryland Hospital for Negro Insane, the hospital opened in 1911 with a complex, sometimes painful history at the intersection of mental health, racism, and institutionalization. Upon the first mention of this project, it was clear that the history of the site was not a backdrop to the project, it was the project.
I started asking questions: how do you design a place where the entire history is a mental health story, and do justice to that story in the ground itself? How do you bridge the gap between clinical conditions and physical outdoor environments?
Those questions have not left me since.
As planners, architects, and landscape architects, we design for health and wellness, for climate resilience, and for equity. Yet somehow, “health and wellness” seems to have become a catch all, to the detriment of being specific. Few resources, conversations, and frameworks in the design world today speak specifically to mental wellness. It has not yet earned that same place in our work.
Meanwhile, a mental health crisis is growing. The National Academies of Sciences, Engineering and Medicine reported in April 2025 that “mental and behavioral health disorders are rising in the U.S. and that preventive interventions need to expand”.
Why, at a time when the need is so great, are many designers still contributing to the taboo of mental health?
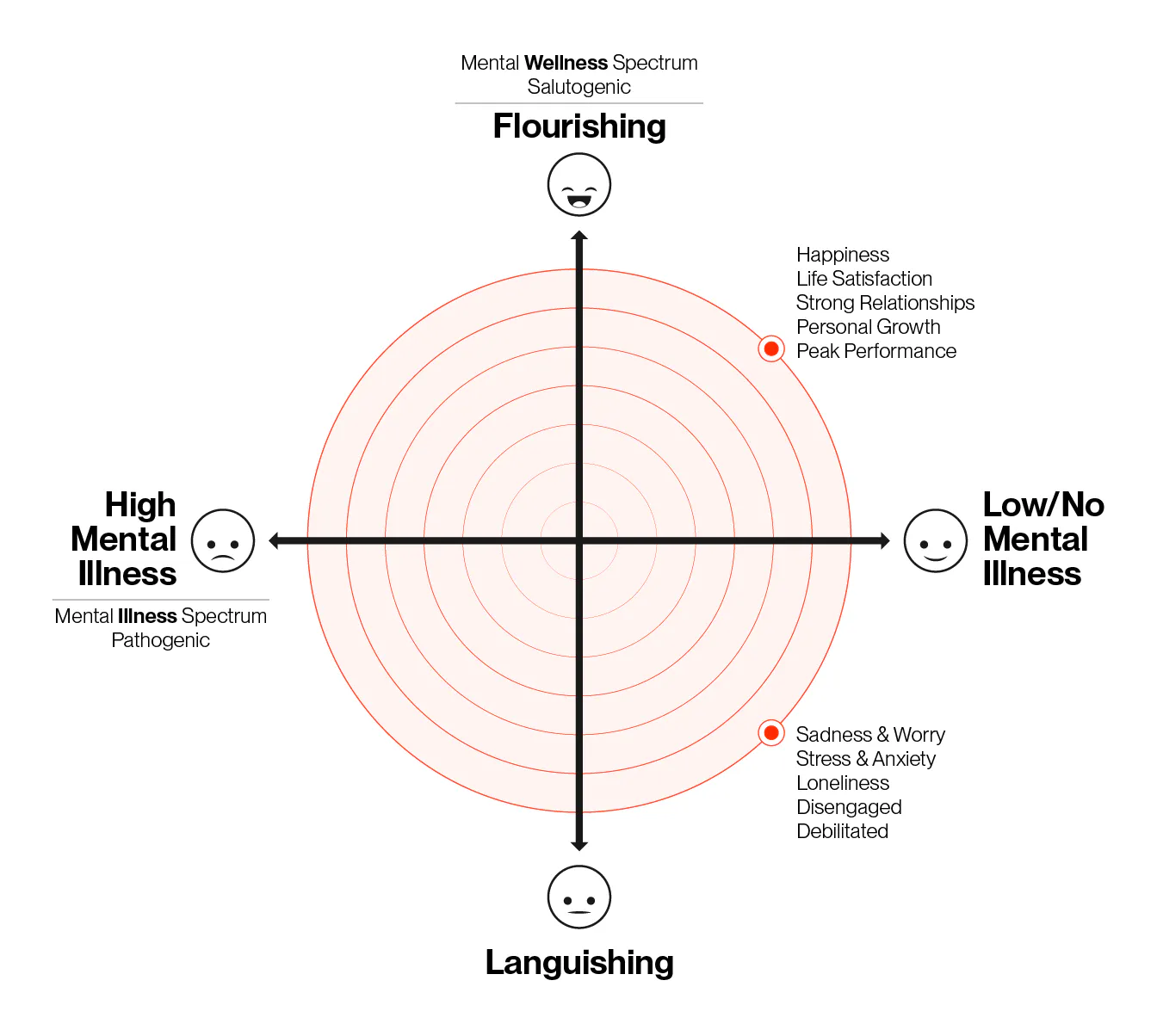
Before we can dive into implementation, we need to understand the language. Mental wellness is more than the absence of mental illness. It is an active, grassroots process: moving from languishing to resilience to flourishing, shifting perspective from stigma to shared humanity. It is multi-dimensional and personal.
Often, we think mental wellness does not apply to our users or us because we are not “mentally ill”. This could not be further from the truth. Incorporating this language into conversations about goals and outcomes of a project takes it to a more specific level, but currently this is absent from the conversation.
{kind=image}
The Delphis Continuum of Mental Health Model is one of many frameworks that can help us with this vocabulary. It names five states people move through: in crisis, struggling, surviving, thriving, excelling. Each comes with concrete indicators. Poor sleep, withdrawal, irritability on one end; flow, energy, fully realizing potential on the other. Once you have those words, you can ask for a project to do something specific. Without them, designing to be "healthy” becomes too vague a goal.
{kind=image}
The research exists. The resources exist. There is rigorous work in academic, non-profit, for-profit, and national institutions to support evidence on how spaces affect our mental wellness. A few resources worth noting, while far from exhaustive are:
- The Centre for Urban Design + Mental Health is a start-up think tank focused on designing better mental health in our cities. The organization publishes the Journal of Urban Design and Mental Health on peer reviewed topics spanning many scales, locations and perspectives on this overlap. (As a personal note, the UD/MH journal was one of the first that sparked my interest in this topic)
- Restorative Cities by Jenny Roe and Layla McCay looks at the city scale and at the evidence base: why it matters, who is affected, what the built environment can change.
- At a more tactical scale, Terrapin Bright Green’s 14 Patterns of Biophilic Design are useful in the room and the site, giving a specific framework for each pattern and how they can directly support physiological stress reduction, cognitive function and performance, and emotion, mood and preference.
With these resources, among many others, we have what we need to design from evidence rather than assumption.
{kind=image}
The question is, how do we bring that evidence into the room from day one, before wellness gets value-engineered out? We’ve seen it before - the budget tightens, the program holds, and the wellness features go first, because the case for them has not been made in measurable terms. If the project goals had named a baseline condition, cited the research connecting specific spatial decisions to belonging and loneliness, and committed to measuring outcomes after occupancy, those same features would have a defense.
This work happens at five levels, starting with the personal one.
The workplace often feels like an “other” place, somewhere feelings are meant to stay behind. I think this stigma is starting to break free. If we want spaces that genuinely support neurodivergence and mental wellness, someone in the room must go first.
Silence in practice starts with silence in ourselves.
Once a month, on Friday, I see a therapist. Hanbury shares calendars across the whole company, and that event is not set to private. It is nonnegotiable for me, and I leave it visible because I think it matters for people to see. If someone notices and decides to do the same, that is enough. If I cannot name what I am doing to take care of my own mental health, I have no place to ask a project to do the same for the people who will use it. It’s not always easy, but the more I do it, the easier it gets.
At level two, the project, the discipline is to ask explicitly: who is this for, and what mental health outcome does this design support?
Then listen first, always. At Crownsville, the most useful conversations were with community members who also worked at the hospital. A former nurse who had worked there gave me the clinical view of what the building had been, and what the site would need to acknowledge before it could become anything else. As designers we are not clinicians and we cannot prescribe. But we can build clinical perspectives into how we engage.
At the public health level, the responsibility is plainer. Placemaking sits at the intersection of the spaces people inhabit and the public health trends shaping their lives. That is not coincidence.
If we cannot talk about it inside our own discipline, how can we solve it anywhere else?
At the firm level, the work is internal. We need conditions where mental health can be named, discussed, and designed for. There have been times when I could see a coworker struggling and did not know how to support them. We need training in this, the same way we train ourselves in any other professional skill.
At the level of our professional organizations, the frameworks we rely on are largely silent on mental health. The WELL Building Standard provides a measurable, criteria-based approach for identifying building features, but stops short of what this means on a larger scale. The American Planning Association (APA) has some of the most substantial research connecting social justice to health and wellness. But across the field, the language stops at "health and wellness." Mental health is typically not specifically named. That is the gap.
And it is a bigger problem than the design profession alone can solve. I have been talking to peers at ASLA and the Landscape Architecture Foundation about exactly this. Not whether mental health gets a page on the website, but whether and how it gets built into how we measure the success of a project.
What would it look like if design for mental wellness were treated with the same rigor as physical health: measurable, evidence-based, embedded into every project phase?
The principles for designing this way are not out of reach. The three below are a starting point, among many others, that are available on every project.
Connection. Spaces that reduce social isolation without forcing interaction. Porches, shared thresholds, programming overlap, community anchors that invite but do not require.
Choice and agency. Users need some control over their environment: noise level, light, privacy, pace. Design that removes choice removes mental wellness benefit. This pushes against the standardizing impulse of large projects, but the evidence behind it is consistent.
Everyday experience. Wellness is not a special trip to a facility. It lives in the daily walk, the porch, the transit station, the pocket park. Design the ordinary with extraordinary care.
{kind=image}
At Crownsville, these principles were realized in design. A deliberately winding path formed the spine of the design, encoding the same truth that healing resists a straight line. Visitors could step off the path and return, engage deeply or pass through lightly, each visit shaped by what they carried that day. Rather than imposing a singular experience, the design made space for the full range of how people move through recovery.
Design for mental wellness is not a clinical afterthought. It is shaped by every spatial decision we make. We design for belonging, autonomy, and repeated positive interaction. Not a single amenity, but a system of moments. The people most affected by environmental stress, those who are disabled, neurodiverse, low-income, BIPOC, are also the people least likely to be asked what they need from a place. That must change in the research, the process, and the outcome.
{kind=image}
Two questions belong at the start of every project: who is this for, and what mental health outcome does this design support? Making the implicit explicit. Then building in choice at every scale: social or solitary, active or restorative, indoors or out, across site, building, unit, landscape, programming.
This is where the work is least developed. But the beginnings of what measurements could look like are emerging quickly, particularly among advancements in technology.
At Virginia Tech, researcher Addison Flack has been using LIDAR to study human occupancy and movement patterns within shared indoor environments, bringing geographic analysis indoors to see where people gather, linger, and overlap. That kind of work points toward what could be possible at the campus scale: studying belonging not as a survey answer but as an observable pattern of where people go and stay.
{kind=image}
Pre- and post-occupancy clinical surveys for anxiety and depression are another component. Sociological observation, being in a space and watching how people use it, is a third. Most of it is qualitative, which makes some clients uncomfortable. That discomfort is part of the point.
Mental wellness does not reduce cleanly to a number, and pretending it does is part of how the topic gets dismissed.
The Landscape Architecture Foundation has built a strong case-study practice around the measurable economic and environmental impacts of projects: stormwater performance, return on investment. I have had early conversations about whether mental wellness outcomes could become a comparable category. The honest answer is we don’t yet know what the measurements are. But figuring it out would change how clients think about their projects, shifting the question from how much stormwater the site captures to how people actually feel in it.
The research is in the room. The resources are in the room. The remaining question is whether we are going to bring them into the brief on day one, or keep cutting them when the budget gets tight.
We cannot have health without mental health. Even quietly, the places we shape, shape us in return.
At the next project kickoff, ask the question out loud: who is this for, and what mental health outcome does this design support? Sit with the silence if it comes. If the room cannot answer, that is the work.
Hanbury has started firmwide discussions about what it means to be a practice that talks openly about mental health. We are still figuring it out. But we are designed to stretch, and this is no exception.
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}
{kind=image}